“The mirror doesn't lie. But it only shows what you're willing to see.”
A mechanic can tell you everything wrong with your car by listening to it idle for thirty seconds.
Not because they're guessing. Because they learned what to hear.
Most people drive past the first rattle, the faint squeal, the subtle pull to one side. They don't notice until the engine light comes on — and by then, the damage has been compounding for months.
Your body has a diagnostic surface too. One you look at every single day.
And once you learn to read it, everything changes.
Your skin reflects your internal health more accurately than any blood test you can see with your eyes. Dermatologists are trained to read it — this card asks you to start learning that language too. The first step isn't treatment. It's honest observation.
The skin is the body's largest organ and its most visible diagnostic surface. Dermatologists can identify liver disease, hormonal imbalance, nutritional deficiency, and stress disorders from skin presentation alone. What you see in the mirror is downstream data from every system in your body.
Disciplines 3 & 4 of 10. New pair tomorrow.
Touch your cheek, forehead, and jawline with clean fingertips. Is the texture the same everywhere? Rough patches, oily zones, and dry spots are diagnostic data your dermatologist would charge to collect.
Look at the skin behind your ears and on the inside of your upper arm — this is the closest to your natural, undamaged skin tone. Compare it to your face. The difference is accumulated environmental damage.
Hormonal fluctuations mean your skin looks different at different points in your cycle. Check mid-cycle (day 14) for your true baseline — not the week before your period when progesterone peaks and sebum increases.
Tap any condition for the full guide — what's happening, what makes it worse, natural approaches that work, and what to do tonight.
Dull Skin (Lack of Radiance)When your skin stops reflecting light the way it used to▸
Skin "glow" is a physics phenomenon. Healthy, well-hydrated skin has a smooth surface that reflects light evenly — producing luminosity. Dull skin has a rough, uneven surface that scatters light in multiple directions, absorbing rather than reflecting.
Three mechanisms create dullness:
1. Dead cell accumulation: desquamation slows with age (by 30-50% between 30 and 80), dehydration, and UV damage. The resulting buildup of corneocytes creates a physical film that scatters light.
2. Dehydration: when the stratum corneum lacks water, cells flatten and curl at the edges, creating an irregular surface. The skin looks matte where it should be luminous.
3. Reduced microcirculation: stress, poor sleep, smoking, and sedentary lifestyle reduce blood flow to the dermis. The pink-toned oxygenated blood beneath the epidermis is what gives healthy skin its warm undertone. Reduced circulation creates the grey, washed-out look of chronically tired skin.
Dehydration — both systemic (not drinking enough) and topical (barrier damage allowing TEWL). Dehydrated cells scatter light instead of reflecting it.
Not exfoliating at all. After 30, desquamation slows enough that dead cells visibly accumulate. Without periodic exfoliation, even well-hydrated skin looks dull because the surface is coated in spent cells.
Smoking reduces dermal blood flow by up to 40%. The grey complexion of smokers is reduced oxygenated haemoglobin showing through depleted skin.
Poor sleep impairs overnight skin repair and reduces growth hormone secretion, which drives cell renewal. The "tired face" is measurably less luminous — quantified in studies using spectrophotometry.
Chemical exfoliation (AHA 5-8%, 2-3 times per week) removes the dead cell layer, revealing the smoother, more reflective surface beneath. Glycolic acid has the smallest molecular weight and penetrates most effectively. Lactic acid is gentler and hydrates simultaneously.
Vitamin C (10-20% L-ascorbic acid) brightens skin through two mechanisms: tyrosinase inhibition (reducing uneven pigmentation) and antioxidant activity (neutralising the free radicals that create the oxidised, yellow-grey tone of dull skin).
Hydration: humectant (glycerin, hyaluronic acid) sealed with occlusive (squalane, shea butter). Well-hydrated cells are plumper, smoother, and more reflective.
Exercise: 20 minutes of moderate activity increases dermal blood flow for 2-4 hours. The "post-exercise glow" is real — increased oxygenated haemoglobin in the dermis is visible through the epidermis.
The "glow" that skincare products promise is primarily the result of exfoliation + hydration. A 5% glycolic acid toner plus a good moisturiser produces more visible luminosity than any "glow serum" at any price.
Dietary carotenoids (from carrots, sweet potatoes, tomatoes) accumulate in the epidermis over weeks, creating a warm, golden undertone. Studies show this carotenoid glow is rated as more attractive than tanned skin.
Blue light from screens doesn't cause dullness directly, but the sleep disruption from late-night screen use does. The correlation people notice between screen time and skin quality is mediated by melatonin suppression and sleep quality.
Skin luminosity varies across the menstrual cycle — oestrogen in the follicular phase (days 1-14) increases dermal blood flow and hydration, creating the "mid-cycle glow." If your skin looks best around ovulation, this is why. The dip in the luteal phase is hormonal, not a product failure.
Dullness on darker skin appears as ashiness — a grey-white cast caused by dead cell accumulation against deeper pigment. The visual impact is often more pronounced than on lighter skin because the contrast between healthy glow and ashy surface is greater.
Gentle exfoliation is key: chemical over physical, to avoid PIH risk. Lactic acid is the safest AHA for darker skin — it exfoliates and hydrates without the irritation risk of glycolic at equivalent concentration.
Apply a gentle AHA product (5% glycolic or 10% lactic acid) to clean, dry skin. Wait 10 minutes, then apply moisturiser. Tomorrow morning, apply vitamin C serum, then moisturiser, then SPF. This three-step combination — exfoliate, brighten, hydrate — produces visible luminosity within 7 days.
Uneven Skin ToneWhen your complexion lacks uniformity▸
An even skin tone means consistent melanin distribution, uniform blood flow visibility, and homogeneous surface texture across the face. Unevenness arises from multiple disruptions to this uniformity:
Pigmentary variation: UV-induced melanin deposits (solar lentigines, freckle clusters), hormonal patches (melasma), and post-inflammatory marks (PIH) create zones of darker pigmentation.
Vascular variation: rosacea, broken capillaries, and areas of chronic inflammation create zones of redness that contrast with surrounding skin.
Sallowness: accumulation of AGEs (from glycation) and reduced microcirculation create a yellow-grey undertone in areas of poor blood flow.
All three types of unevenness share a common amplifier: UV exposure. Every mechanism that creates uneven tone is worsened by UV and improved by photoprotection.
UV exposure is the primary driver — it darkens existing hyperpigmentation, creates new spots, damages blood vessels (increasing redness), and accelerates glycation (increasing sallowness). Without daily SPF, no treatment for uneven tone can maintain results.
Inconsistent skincare: treating some areas of the face but not others creates visible differences in texture and luminosity.
Smoking: the combination of reduced blood flow (pallor) and increased glycation (yellowing) creates the characteristic "smoker's complexion" — grey and sallow.
Skipping exfoliation: accumulated dead cells scatter light unevenly, making underlying pigmentation differences more pronounced.
Vitamin C (15-20% L-ascorbic acid) is the most evidence-based tone-evening agent. It inhibits tyrosinase (reducing pigmentation), neutralises free radicals (reducing sallowness), and supports collagen synthesis. Applied daily for 8-12 weeks, it produces measurable improvement in overall tone evenness.
Niacinamide (5%) blocks melanosome transfer, reducing the delivery of excess melanin to keratinocytes. It also reduces redness through anti-inflammatory activity — addressing both pigmentary and vascular unevenness.
AHA (glycolic 5-8%) exfoliates unevenly pigmented surface cells, revealing a more uniform layer beneath. The mechanical removal of pigmented cells accelerates what cell turnover would eventually accomplish.
Azelaic acid (15-20%) preferentially targets overactive melanocytes, leaving normal pigmentation untouched. Uniquely useful for patchy, asymmetric tone issues.
SPF 30+ daily. This is the foundation — every other treatment fails without it.
Tone evenness contributes more to perceived attractiveness than specific skin colour. Studies show that uniform colour distribution is rated as healthier and more attractive than lighter or darker skin per se.
Dietary carotenoids (beta-carotene from carrots and sweet potatoes, lycopene from tomatoes) create a warm, even undertone when they accumulate in the epidermis. Research shows this carotenoid glow is rated as more attractive than a suntan.
The "glass skin" trend is fundamentally about tone evenness + hydration. No product creates it. Consistent SPF + vitamin C + hydration over months does.
Hormonal transitions (menstruation, pregnancy, perimenopause) all affect melanocyte activity and blood vessel reactivity, creating temporary unevenness. Tone that varies with your cycle is hormonal — consistent SPF and vitamin C maintain the best baseline across hormonal fluctuations.
Uneven tone is the number one aesthetic concern reported by women of colour. The higher melanocyte reactivity in Fitzpatrick IV-VI skin means every inflammatory event, hormonal shift, and UV exposure creates more pronounced pigmentary variation.
Treatment requires patience and gentleness. Aggressive brightening agents on darker skin can cause irritation that triggers more PIH — worsening the original unevenness. Start low-concentration, build slowly.
Apply vitamin C serum to the entire face (not spot-treating — even application is the point). If you don't have vitamin C, use niacinamide serum across the full face. Tomorrow morning: SPF everywhere, including the ears and neck. The evenness protocol is full-face antioxidant + full-face SPF, every day. The consistency creates the uniformity.
Dark Under-Eye CirclesWhen tiredness writes itself beneath your eyes▸
Dark circles have three distinct causes — and most people have more than one operating simultaneously.
Vascular: the skin under the eyes is the thinnest on the face (0.5mm vs 2mm elsewhere). Blood vessels beneath this translucent skin are visible as blue-purple shadows. Poor circulation, nasal congestion (allergic shiners), and vasodilation from fatigue all increase the visibility of these vessels.
Pigmentary: melanin deposition in the periorbital skin, caused by genetics, sun exposure, post-inflammatory hyperpigmentation, or hormonal changes. More common in Fitzpatrick III-VI skin. Appears brown rather than blue-purple.
Structural: as orbital fat pads thin with age (or are genetically thin), the hollow beneath the eye deepens, creating a shadow that looks like darkness. This is a volume loss problem, not a colour problem — and no topical product addresses it because the issue is architectural, not pigmentary.
Most under-eye darkness is a combination of all three. Identifying the dominant type determines which intervention works.
Sleep deprivation dilates periorbital blood vessels and reduces lymphatic drainage — making vascular dark circles measurably worse within a single night. The effect persists for 48-72 hours after recovery sleep.
Allergies cause nasal congestion, which restricts venous drainage from the periorbital area, pooling deoxygenated blood beneath the thin skin. Antihistamines reduce allergic shiners within days.
UV exposure increases melanin deposition in the periorbital skin — and this area is the most commonly skipped during SPF application. Sunglasses provide physical protection that no cream replicates.
Rubbing the eyes (from allergies, fatigue, or habitual touching) creates mechanical irritation that triggers PIH in susceptible skin. The friction itself becomes a cause.
For vascular circles: caffeine topically (1-5%) constricts blood vessels temporarily, reducing the blue-purple appearance for 4-8 hours. Cold compresses (or chilled tea bags — the tannins are mildly vasoconstrictive) reduce puffiness and vessel dilation. Sleep is the most effective vascular intervention — 7-8 hours consistently.
For pigmentary circles: vitamin C (10-15%) inhibits tyrosinase and gradually lightens melanin deposits over 8-12 weeks. Niacinamide (5%) blocks melanosome transfer. Vitamin K cream has limited but promising evidence for reducing vascular-pigmentary hybrid circles.
For structural circles: no topical product restores lost orbital fat volume. Retinol can thicken the epidermis slightly (making vessels less visible), but true structural hollows require dermal filler or acceptance. Honest expectation-setting matters here.
SPF + sunglasses daily prevent worsening of all three types.
The "darkness" under your eyes may not be colour at all — it may be shadow. Take a photo in flat, diffused light (like an overcast day). If the circles nearly disappear, the cause is structural (hollowing), not pigmentary. No cream fixes a shadow.
Iron deficiency makes vascular dark circles visibly worse. Low iron reduces haemoglobin oxygen saturation, making the blood pooling under the eyes appear darker. If circles persist despite sleep and hydration, check your ferritin levels.
Retinol is the only topical proven to thicken periorbital skin (increasing epidermal density), which makes underlying vessels less visible. The effect takes 12+ weeks but is the closest thing to a structural topical fix.
Hormonal fluctuations affect under-eye circles — oestrogen influences vascular dilation and fluid retention, making circles more visible premenstrually and during pregnancy. Iron deficiency (common in menstruating women) compounds the vascular component. If circles are cyclical, the hormone connection is active.
Periorbital hyperpigmentation is among the most common dermatological concerns in Fitzpatrick IV-VI skin. The melanin-driven component is dominant — not vascular — meaning brightening agents (vitamin C, niacinamide, azelaic acid) are more effective than vasoconstrictors.
Bleaching agents around the eyes require extreme caution: the skin is thin, absorption is higher, and irritation risk (leading to more PIH) is elevated. Start any brightening product at half the facial concentration.
Apply a caffeine-containing eye product or place two chilled spoons on your closed eyes for 5 minutes (vasoconstriction). Then apply a vitamin C or retinol eye cream. Tomorrow: SPF around the eyes AND sunglasses. The combination addresses all three mechanisms — vascular, pigmentary, and structural — simultaneously.
Chronic Dehydrated SkinWhen the wall is leaking water▸
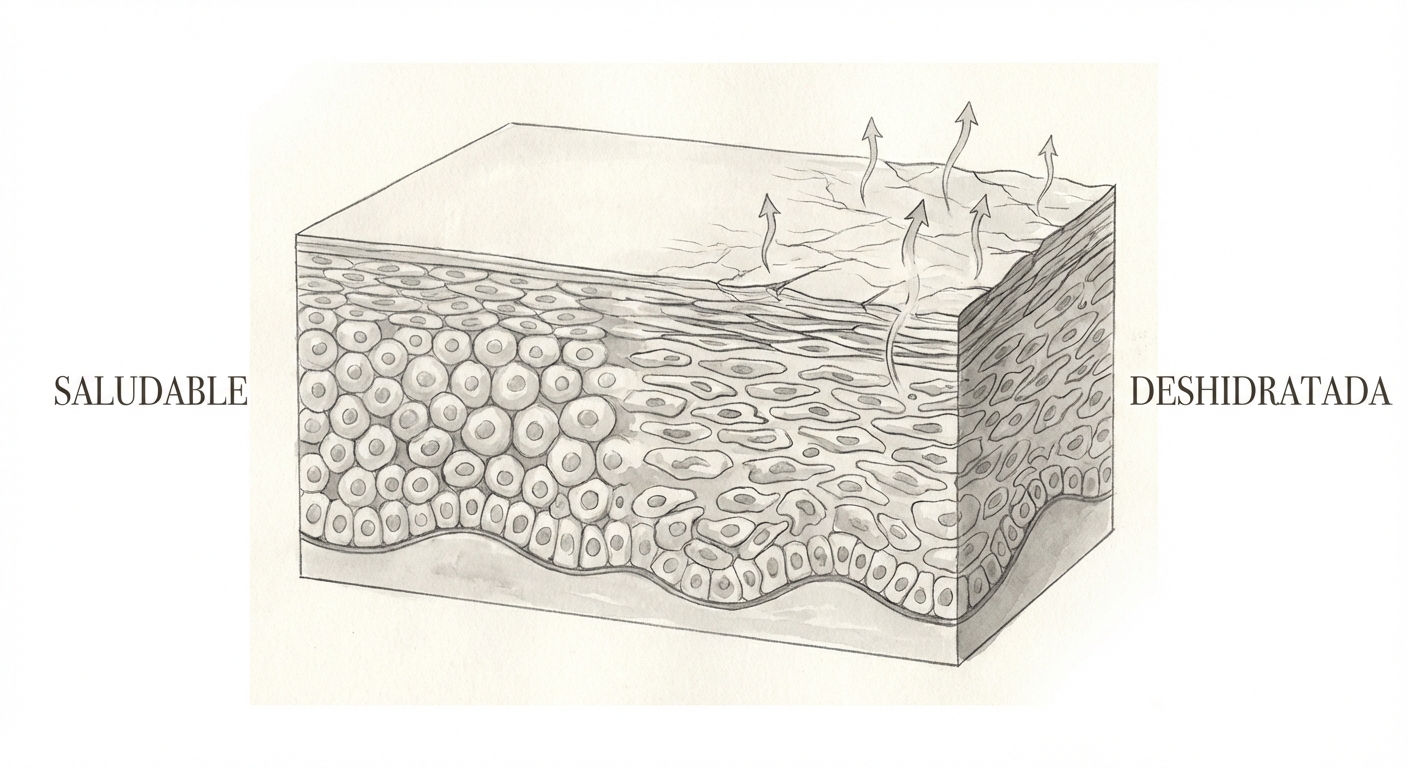
Dehydration is different from dryness. Dry skin is a type — your sebaceous glands produce less oil. Dehydrated skin is a condition — your stratum corneum lacks water. You can have oily, dehydrated skin simultaneously.
Your skin gets its water from the dermis upward, not from drinking water. The stratum corneum retains water through two mechanisms: the lipid mortar (ceramides, cholesterol, fatty acids) prevents evaporation, and the Natural Moisturising Factor (NMF) — a cocktail of amino acids, lactate, urea, and PCA inside corneocytes — holds water like a sponge.
When either is depleted, transepidermal water loss (TEWL) increases. Water evaporates from the surface faster than it's delivered from below. The skin looks dull, feels tight, and shows fine dehydration lines that disappear when pressed.
SLS-containing cleansers strip both the lipid mortar AND the water-soluble NMF components simultaneously — a double hit.
Hyaluronic acid can make dehydration worse in dry climates. HA is a humectant that attracts water from wherever it can find it. Below ~40% humidity (most heated or air-conditioned interiors in winter), HA pulls water from your deeper dermis to the surface, where it evaporates. Without an occlusive on top, HA acts as a wick drawing water OUT of your skin.
Alcohol-based toners cause instant TEWL spikes. Hot water dissolves the lipid barrier. Aggressive exfoliation removes corneocytes before their NMF payload is metabolised.
The fix is two-step: humectant (attracts water) then occlusive (prevents loss).
Humectants: honey contains glycerol and amino acids with humectant activity, plus antimicrobial properties. Aloe vera is humectant via mucopolysaccharides plus anti-inflammatory. Glycerin — already present in your skin as an NMF breakdown product — is one of the most evidence-supported humectants and is inexpensive.
Occlusives: shea butter (37.8% TEWL reduction in 24 hours). Beef tallow (fatty acid profile matches SC lipids, good occlusion — but can be comedogenic for some). Squalane (plant-derived, light occlusion, excellent tolerance). Plain petroleum jelly (the most effective occlusive available, zero comedogenic risk on compromised skin).
The key: apply humectant to DAMP skin, then seal with occlusive immediately. Without the seal, the humectant pulls water to the surface and lets it evaporate.
Drinking water doesn't meaningfully hydrate your skin. The skin receives water from the dermis upward through the epidermis — systemic hydration via drinking can't compensate for a defective barrier that's losing water faster than it's delivered. A leaking roof isn't fixed by adding more water to the tank.
Your NMF is stripped every time you wash with a surfactant cleanser. Morning face wash may be unnecessary — if you weren't sweating overnight, a water-only rinse preserves NMF.
The "pinch test" can detect dehydration: gently pinch cheek skin. Dehydrated skin shows fine horizontal lines and returns to normal slightly slower.
Women experience more cyclical dehydration linked to the menstrual cycle. Progesterone is mildly diuretic — the luteal phase brings some reduction in skin hydration before menstruation. If your skin reliably feels drier in the week before your period, this is hormonal, not imagined.
Darker skin tones have measurably higher TEWL and lower ceramide content as a natural baseline compared to lighter skin (Rawlings 1994 and subsequent studies). Xerosis on Fitzpatrick IV-VI skin appears ashen or "grey-looking" against deeper pigment — more socially visible and more stigmatised. Dehydration in darker skin carries both a physiological and psychosocial burden.
After washing, while skin is still damp, press a thin layer of glycerin (diluted to 3-10% with water) or aloe vera onto your face, then immediately apply shea butter, squalane, or petroleum jelly. This humectant → occlusive sequence on damp skin is the single most evidence-supported approach to rapid rehydration. Two steps. Two minutes.
Photoaged Skin (Premature Wrinkles & Laxity)When decades of UV exposure arrive on your face at once▸
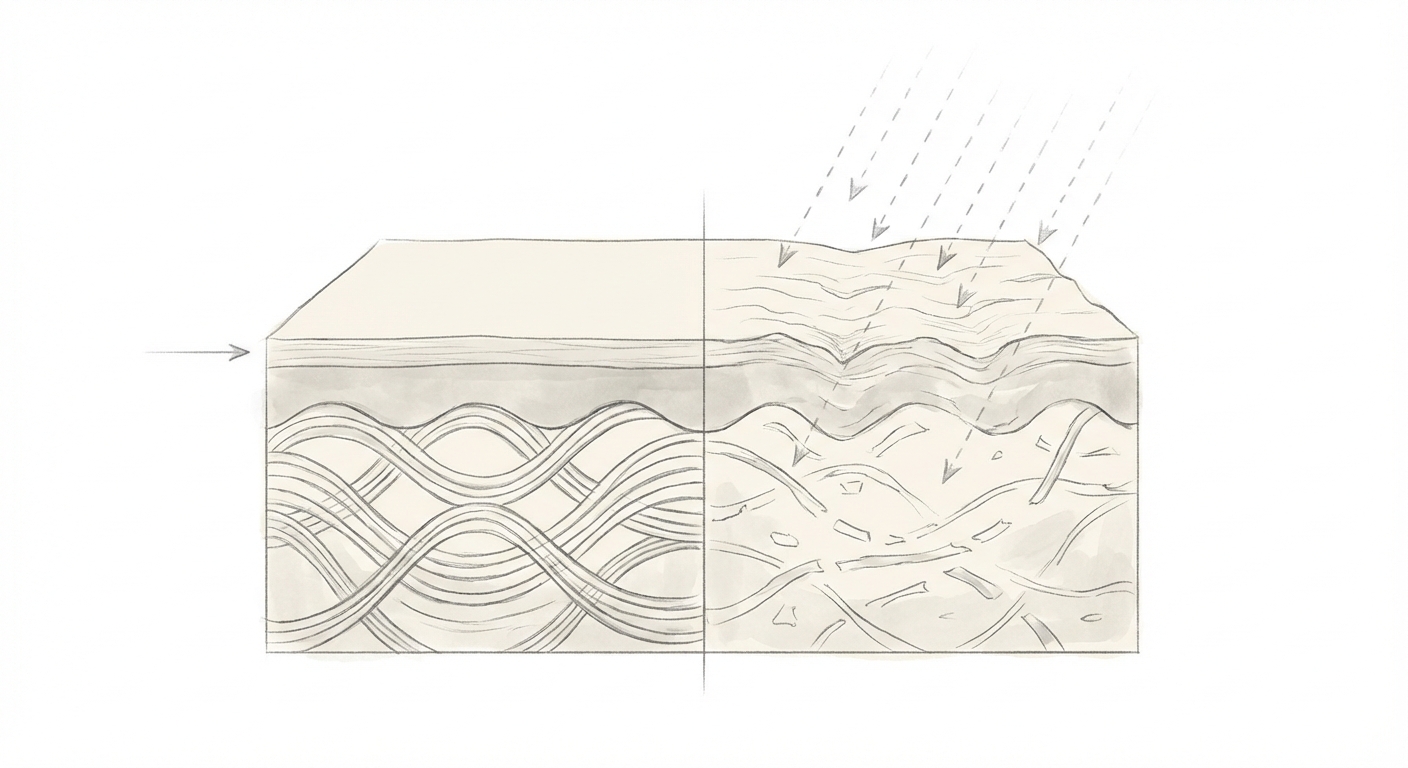
Photoaging is structurally different from chronological (intrinsic) ageing. Chronological ageing produces fine, even wrinkles with skin thinning. Photoaging produces deep, coarse wrinkles with thickened, leathery skin — a condition dermatologists call solar elastosis.
The mechanism: UVA generates reactive oxygen species (ROS) that activate matrix metalloproteinases (MMPs) — enzymes that break down collagen type I and III, and degrade elastin fibres. Each UV exposure episode generates MMPs that persist for 24-48 hours. Over years, the cumulative collagen loss creates permanent structural collapse: wrinkles, furrows, and sagging.
Simultaneously, damaged elastin fibres clump into non-functional masses (solar elastosis), producing the thickened, yellowish, inelastic texture characteristic of chronic sun damage. This is most visible on the neck, décolletage, and backs of hands.
Incidental daily UV does more cumulative damage than holiday sunburns. A 15-minute commute, 5 days a week, 48 weeks a year = 60 hours of annual UV exposure — more than a two-week beach holiday. And most people don't wear SPF for the commute.
Smoking accelerates photoaging multiplicatively: UV + smoking produces more MMP activation than either alone. The combination creates the deepest perioral wrinkles (around the mouth) through both UV damage and repeated pursing.
Retinol without SPF is counterproductive: retinol increases photosensitivity by accelerating cell turnover. Newer, thinner cells are more UV-vulnerable. Using retinol at night and skipping SPF in the morning is like sanding the floor and then dragging furniture across it.
Daily broad-spectrum SPF 30+ prevents further damage accumulation. The Queensland study proved this is the single most effective anti-ageing intervention available — superior to any product at any price.
Retinol (0.3-1%) is the most evidence-supported topical for reversing existing photoaging. It stimulates collagen synthesis, increases cell turnover, and reorganises the dermal matrix. Kligman et al. demonstrated measurable improvement in fine lines, texture, and pigmentation over 24 weeks.
Vitamin C (15-20% L-ascorbic acid) neutralises UV-generated ROS and is a required cofactor for collagen synthesis. Applied in the morning under SPF, it provides antioxidant photoprotection + collagen support.
Niacinamide (5%) improves skin elasticity, reduces yellowing (solar elastosis), and decreases hyperpigmentation in photoaged skin. It's the most tolerable active for mature, photodamaged skin.
Omega-3 (oral, 2g/day EPA+DHA) reduces UV-induced MMP expression. A 2013 study found omega-3 supplementation reduced sunburn sensitivity by 2×, indicating reduced inflammatory response to UV.
The difference between a 55-year-old who wore daily SPF from 30 and one who didn't is approximately 10 years of visible ageing. The "good genetics" you admire in people who age well is usually "good SPF habits."
Photoaging is asymmetric: the left side of the face (in right-hand-drive countries) or the right side (in left-hand-drive countries) shows more photodamage due to UV through car windows during daily commutes. If one side of your face looks older, this is why.
Retinol works on photoaged skin at any age. Studies in 60+ year old patients show measurable improvement. The fibroblasts haven't stopped working — they just need the stimulus. It is never too late to start.
Post-menopausal women experience a double hit: intrinsic collagen loss from oestrogen decline (up to 30% in 5 years) combined with cumulative photoaging. The acceleration of visible ageing around menopause is the intersection of these two independent processes. Retinol + SPF + niacinamide addresses both pathways.
Melanin provides a natural SPF equivalent of approximately 2-4 in Fitzpatrick IV-VI skin — protective but not sufficient. Photoaging in darker skin presents as mottled hyperpigmentation, textural roughness, and dermatosis papulosa nigra (small dark papules) rather than the wrinkles and laxity pattern seen in lighter skin.
The misconception that "dark skin doesn't need sunscreen" leads to late-stage photoaging and higher rates of UV-related pigmentary disorders. SPF is essential for all skin tones — the ageing pattern differs, the damage doesn't.
Apply retinol tonight (start at 0.3% if new to it, or use your current strength). Tomorrow morning, apply vitamin C serum, then SPF 30+. This AM/PM combination — antioxidant + SPF by day, retinol by night — is the most evidence-supported anti-photoaging routine that exists. Two steps, twice a day, every day.
▸Sources & how we research
Our research principles
The content on this page draws from peer-reviewed dermatological research (PubMed, PMC), regulatory positions (FDA, EU SCCS, IARC), and the investigative work of Dr. Samuel Epstein (Safe Shopper's Bible, Toxic Beauty) on harmful ingredients in commercial products.
Where we recommend natural alternatives, we cite the evidence level honestly. Colloidal oatmeal has multiple double-blind RCTs. Jojoba oil has clinical trials. Beef tallow has mechanistic evidence and a 2024 scoping review but no human RCTs. We distinguish between “proven” and “biologically plausible” — and we tell you which is which.
We avoid the EWG Skin Deep database as a primary source. Approximately 80% of Society of Toxicology members consider it overstates chemical risks. It conducts hazard assessment without dose-response analysis — the foundational principle of toxicology. We use it as an investigative starting point, not a definitive authority.
The Solfeggio frequency labels on our sister deck carry an attribution note explaining their 1999 origin. We apply the same standard here: where the evidence is strong, we say so. Where it's emerging, traditional, or anecdotal, we say that too.
This content is educational, not medical advice. If you have a persistent skin condition, see a dermatologist. We are not doctors — we are researchers who believe you deserve honest information about what touches your skin.
Instant diagnosis and personalised tips.